Review Sheet 31 Conduction System of the Heart
The most continuous traffic into and out of a busy mill at rush hour occurs at a snails' stride compared to the endless activity going on inside our bodies. Like the bustling mill, the body must have a transportation system to carry its various cargos back and forth, and this is where the cardiovascular system steps in.
Functions of the Heart
The functions of the heart are every bit follows:
- Managing blood supply. Variations in the rate and strength of heart contraction match claret menses to the changing metabolic needs of the tissues during rest, exercise, and changes in body position.
- Producing blood pressure. Contractions of the middle produce claret force per unit area, which is needed for claret catamenia through the blood vessels.
- Securing ane-style blood period. The valves of the middle secure a 1-style claret menses through the centre and blood vessels.
- Transmitting blood. The centre separates the pulmonary and systemic circulations, which ensures the flow of oxygenated claret to tissues.
Anatomy of the Center
The cardiovascular system can be compared to a muscular pump equipped with one-way valves and a system of big and modest plumbing tubes within which the blood travels.
Centre Structure and Functions
The modest size and weight of the heart give few hints of its incredible strength.
- Weight. Approximately the size of a person's fist, the hollow, cone-shaped heart weighs less than a pound.
- Mediastinum. Snugly enclosed within the inferior mediastinum, the medial cavity of the thorax, the heart is flanked on each side by the lungs.
- Noon. It'south more pointed apex is directed toward the left hip and rests on the diaphragm, approximately at the level of the 5th intercostal space.
- Base of operations. Its broad posterosuperior aspect, or base, from which the dandy vessels of the body sally, points toward the right shoulder and lies beneath the 2d rib.
- Pericardium. The heart is enclosed in a double-walled sac called the pericardium and is the outermost layer of the centre.
- Fibrous pericardium. The loosely fitting superficial part of this sac is referred to every bit the fibrous pericardium, which helps protect the centre and anchors it to surrounding structures such as the diaphragm and sternum.
- Serous pericardium. Deep to the fibrous pericardium is the slippery, 2-layer serous pericardium, where its parietal layer lines the interior of the fibrous pericardium.
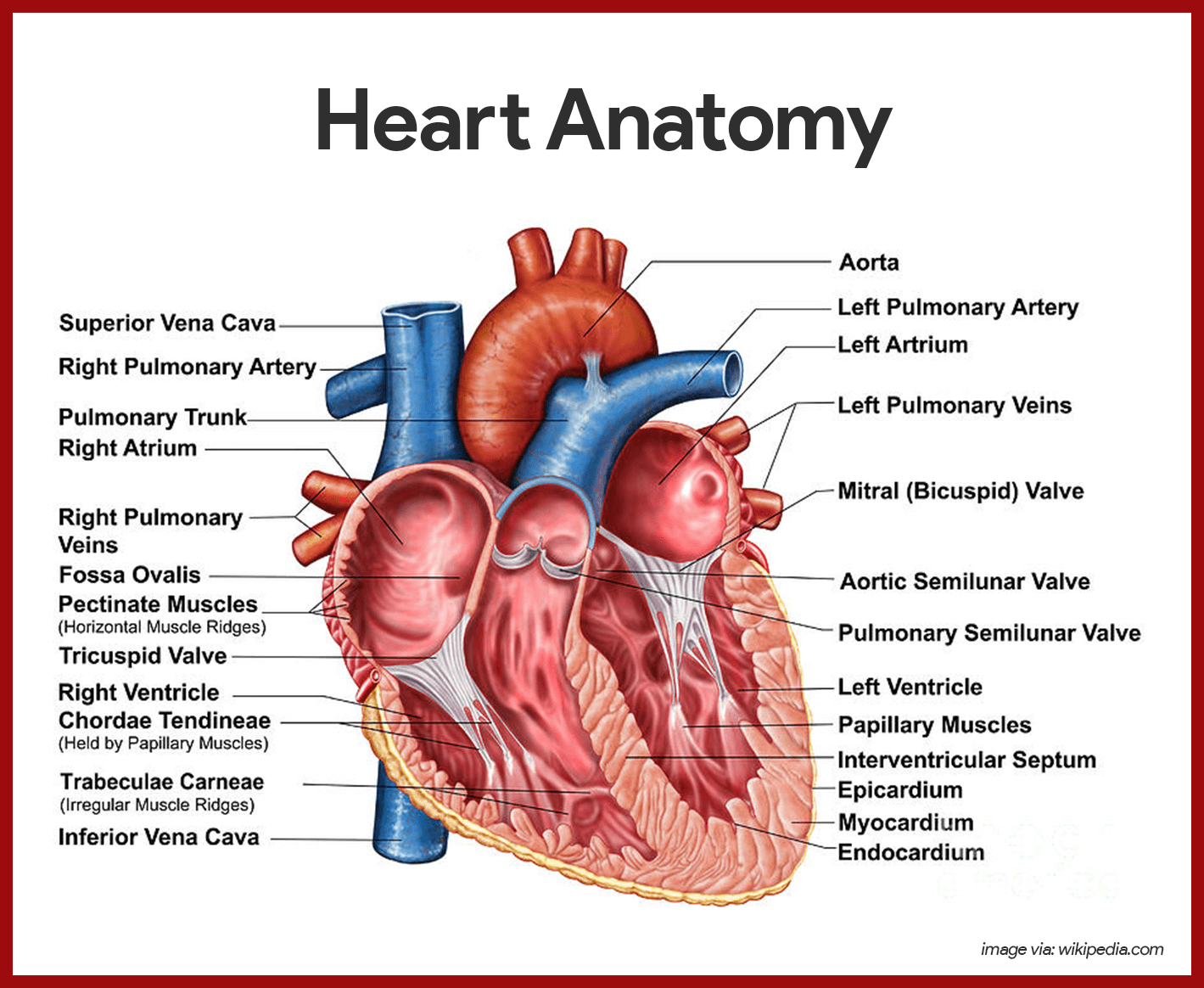
Layers of the Centre
The center musculus has three layers and they are as follows:
- Epicardium. The epicardium or the visceral and outermost layer is actually a role of the eye wall.
- Myocardium. The myocardium consists of thick bundles of cardiac muscle twisted and whirled into ringlike arrangements and information technology is the layer that really contracts.
- Endocardium. The endocardium is the innermost layer of the heart and is a thin, glistening sheet of endothelium hat lines the heart chambers.
Chambers of the Middle
The heart has 4 hollow chambers, or cavities: two atria and two ventricles.
- Receiving chambers. The two superior atria are primarily the receiving chambers, they play a lighter role in the pumping activeness of the middle.
- Discharging chambers. The two inferior, thick-walled ventricles are the discharging chambers, or bodily pumps of the heart wherein when they contract, blood is propelled out of the heart and into the apportionment.
- Septum. The septum that divides the middle longitudinally is referred to as either the interventricular septum or the interatrial septum, depending on which bedroom it separates.
Associated Great Vessels
The great blood vessels provide a pathway for the unabridged cardiac apportionment to proceed.
- Superior and inferior vena cava. The centre receives relatively oxygen-poor blood from the veins of the body through the large superior and inferior vena cava and pumps it through the pulmonary trunk.
- Pulmonary arteries. The pulmonary trunk splits into the correct and left pulmonary arteries, which deport blood to the lungs, where oxygen is picked upwardly and carbon dioxide is unloaded.
- Pulmonary veins. Oxygen-rich claret drains from the lungs and is returned to the left side of the heart through the four pulmonary veins.
- Aorta. Claret returned to the left side of the middle is pumped out of the centre into the aorta from which the systemic arteries branch to supply essentially all body tissues.
Heart Valves
The heart is equipped with iv valves, which allow blood to flow in only one direction through the center chambers.
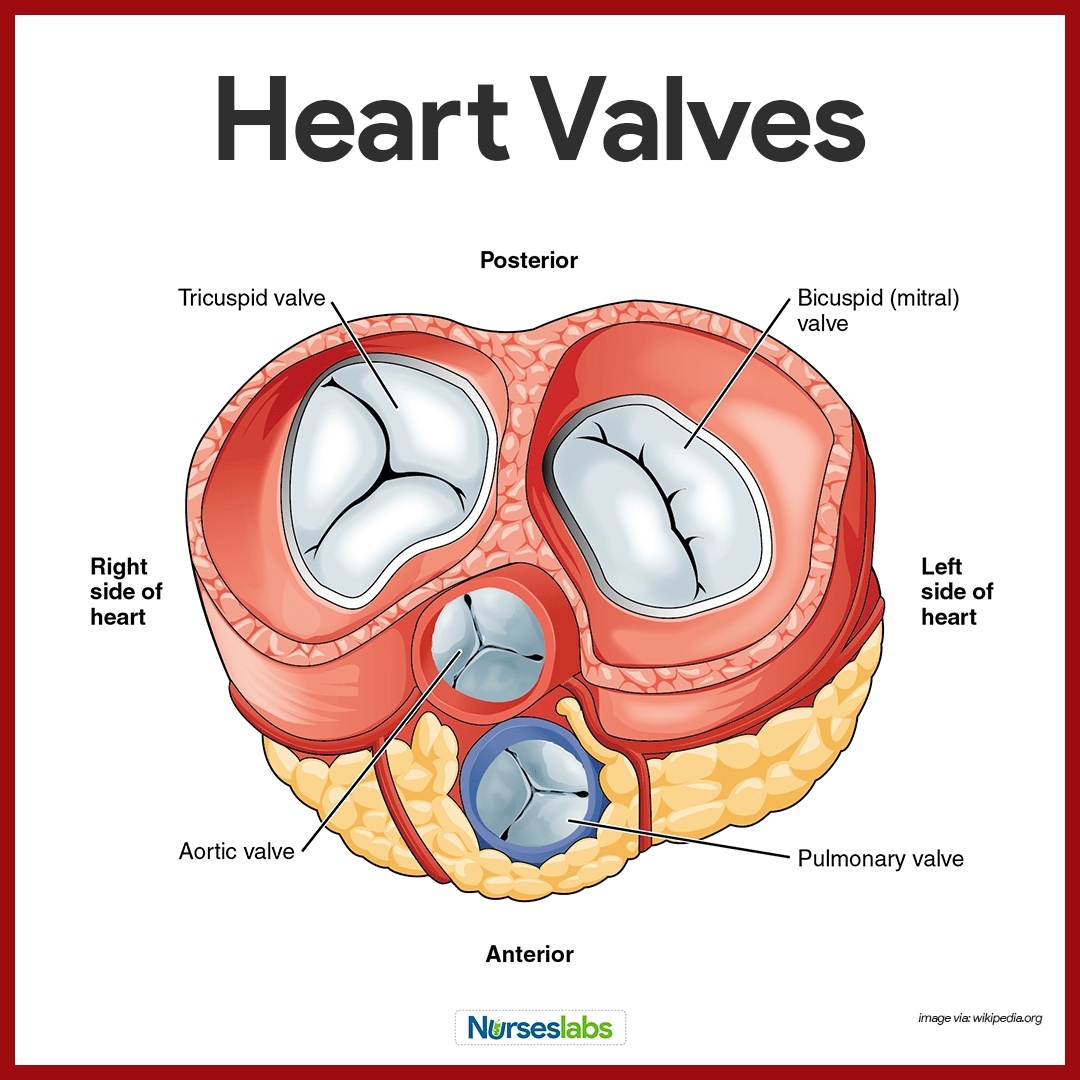
- Atrioventricular valves. Atrioventricular or AV valves are located between the atrial and ventricular chambers on each side, and they prevent backflow into the atria when the ventricles contract.
- Bicuspid valves. The left AV valve- the bicuspid or mitral valve, consists of two flaps, or cusps, of endocardium.
- Tricuspid valve. The correct AV valve, the tricuspid valve, has iii flaps.
- Semilunar valve. The 2nd set of valves, the semilunar valves, guards the bases of the two large arteries leaving the ventricular chambers, thus they are known as the pulmonary and aortic semilunar valves.
Cardiac Apportionment Vessels
Although the heart chambers are bathed with blood almost continuously, the claret independent in the heart does not nourish the myocardium.
- Coronary arteries. The coronary arteries branch from the base of the aorta and encircle the heart in the coronary sulcus (atrioventricular groove) at the junction of the atria and ventricles, and these arteries are compressed when the ventricles are contracting and fill when the heart is relaxed.
- Cardiac veins. The myocardium is drained by several cardiac veins, which empty into an enlarged vessel on the posterior of the middle called the coronary sinus.
Blood Vessels
Claret circulates inside the claret vessels, which form a airtight transport system, the then-chosen vascular system.
- Arteries. Equally the eye beats, blood is propelled into large arteries leaving the heart.
- Arterioles. Information technology then moves into successively smaller and smaller arteries and and so into arterioles, which feed the capillary beds in the tissues.
- Veins. Capillary beds are tuckered by venules, which in plow empty into veins that finally empty into the bang-up veins entering the heart.
Tunics
Except for the microscopic capillaries, the walls of the blood vessels have iii coats or tunics.
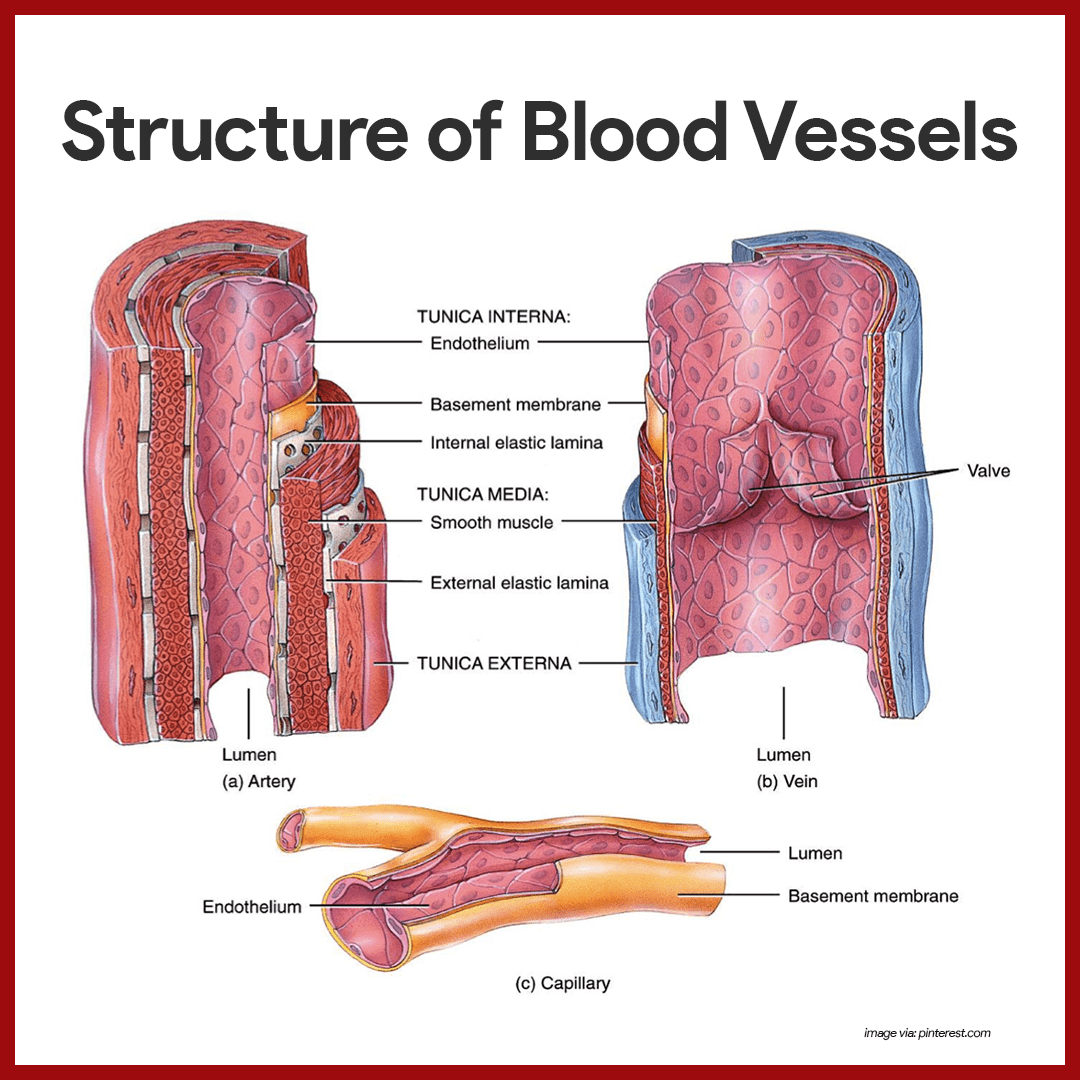
- Tunica intima. The tunica intima, which lines the lumen, or interior, of the vessels, is a thin layer of endothelium resting on a basement membrane and decreases friction as blood flows through the vessel lumen.
- Tunica media. The tunica media is the bulky center coat which mostly consists of shine muscle and elastic fibers that tuck or amplify, making the blood pressure level increase or decrease.
- Tunica externa. The tunica externa is the outermost tunic composed largely of fibrous connective tissue, and its role is basically to support and protect the vessels.
Major Arteries of the Systemic Circulation
The major branches of the aorta and the organs they serve are listed next in sequence from the heart.
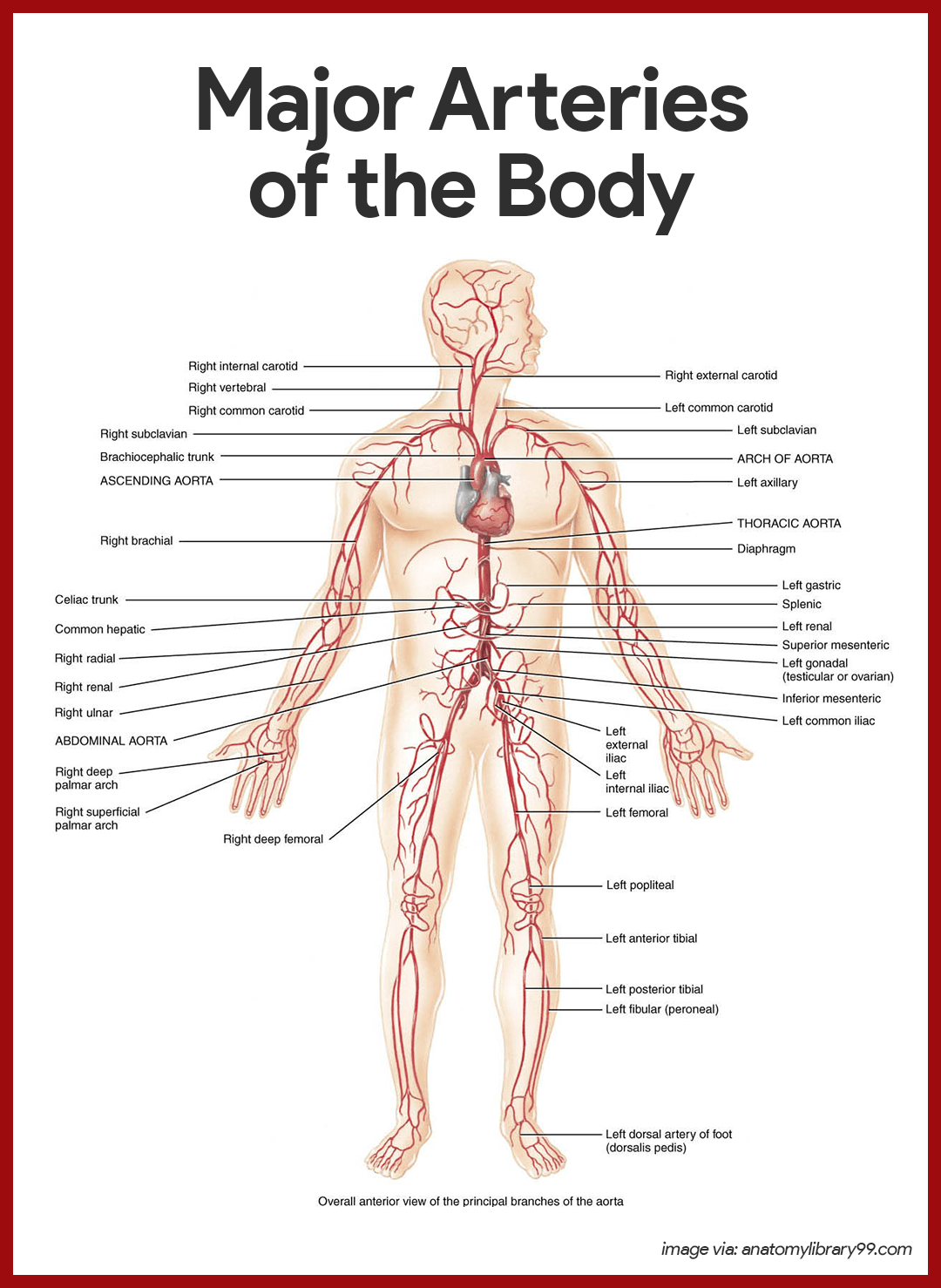
Arterial Branches of the Ascending Aorta
The aorta springs upwardly from the left ventricle of middle as the ascending aorta.
- Coronary arteries. The simply branches of the ascending aorta are the right and left coronary arteries, which serve the heart.
Arterial Branches of the Aortic Arch
The aorta arches to the left as the aortic curvation.
- Brachiocephalic trunk. The brachiocephalic trunk, the first branch off the aortic curvation, splits into the right common carotid avenue and right subclavian artery.
- Left common carotid artery. The left common carotid artery is the 2d branch off the aortic curvation and it divides, forming the left internal carotid, which serves the brain, and the left external carotid, which serves the skin and muscles of the caput and neck.
- Left subclavian artery. The third branch of the aortic arch, the left subclavian artery, gives off an important co-operative- the vertebral artery, which serves function of the brain.
- Axillary artery. In the axilla, the subclavian avenue becomes the axillary artery.
- Brachial artery. the subclavian artery continues into the arm every bit the brachial avenue, which supplies the arm.
- Radial and ulnar arteries. At the elbow, the brachial artery splits to grade the radial and ulnar arteries, which serve the forearm.
Arterial Branches of the Thoracic Aorta
The aorta plunges downward through the thorax, following the spine as the thoracic aorta.
- Intercostal arteries. Ten pairs of intercostal arteries supply the muscles of the thorax wall.
Arterial Branches of the Intestinal Aorta
Finally, the aorta passes through the diaphragm into the abdominopelvic cavity, where it becomes the abdominal aorta.
- Celiac torso. The celiac trunk is the first branch of the abdominal aorta and has three branches: the left gastric artery supplies the stomach; the splenic avenue supplies the spleen, and the common hepatic avenue supplies the liver.
- Superior mesenteric artery. The unpaired superior mesenteric avenue supplies most of the pocket-size intestine and the first half of the large intestine or colon.
- Renal arteries. The renal arteries serve the kidneys.
- Gonadal arteries. The gonadal arteries supply the gonads, and they are chosen ovarian arteries in females while in males they are testicular arteries.
- Lumbar arteries. The lumbar arteries are several pairs of arteries serving the heavy muscles of the abdomen and trunk walls.
- Inferior mesenteric artery. The inferior mesenteric artery is a small, unpaired artery supplying the second half of the large intestine.
- Common iliac arteries. The common iliac arteries are the terminal branches of the abdominal aorta.
Major Veins of the Systemic Apportionment
Major veins converge on the venae cavae, which enter the right atrium of the heart.
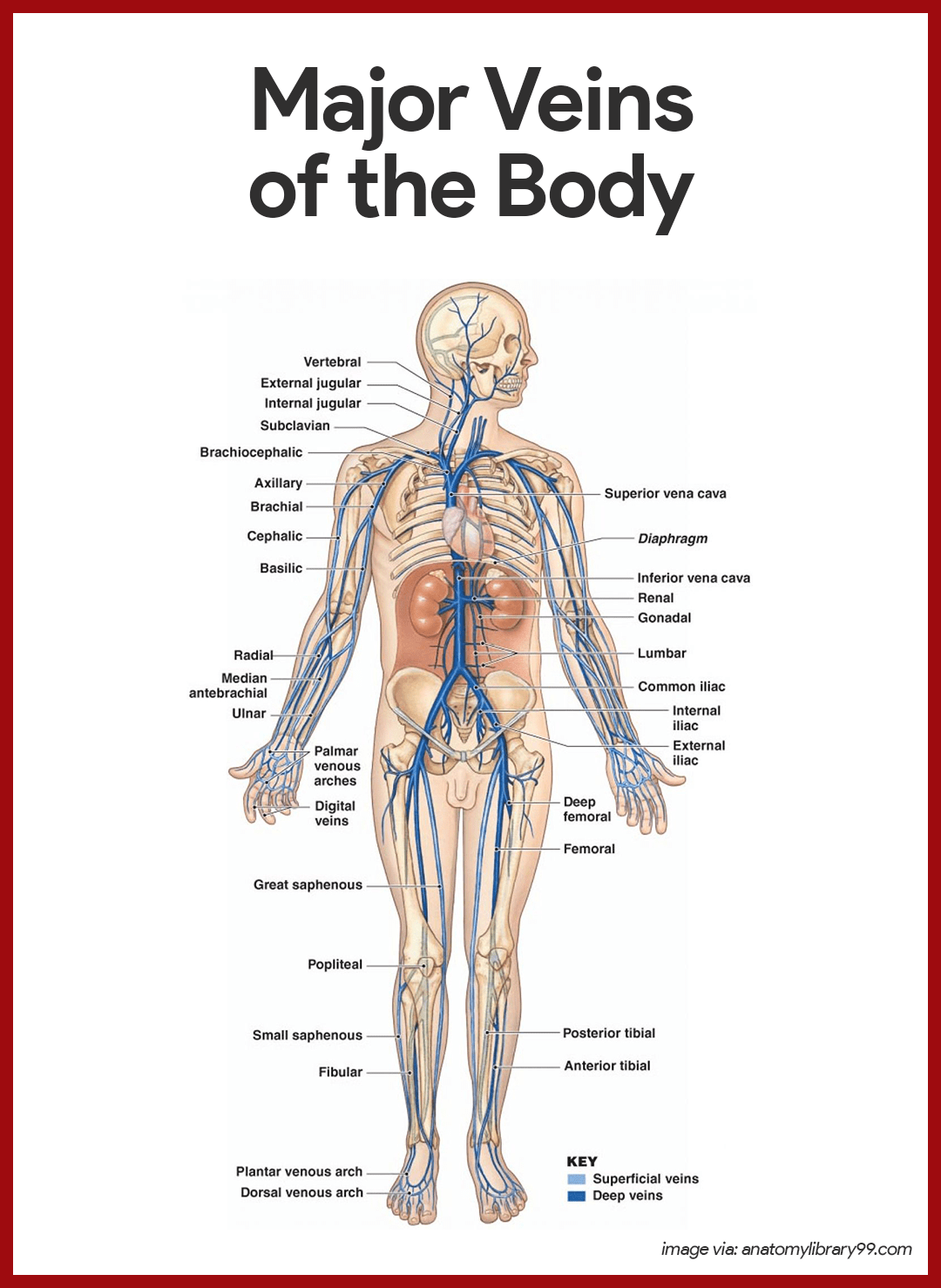
Veins Draining into the Superior Vena Cava
Veins draining into the superior vena cava are named in a distal-to-proximal direction; that is, in the same direction the claret flows into the superior vena cava.
- Radial and ulnar veins. The radial and ulnar veins are deep veins draining the forearm; they unite to class the deep brachial vein, which drains the arm and empties into the axillary vein in the axillary region.
- Cephalic vein. The cephalic vein provides for the superficial drainage of the lateral attribute of the arm and empties into the axillary vein.
- Basilic vein. The basilic vein is a superficial vein that drains the medial aspect of the arm and empties into the brachial vein proximally.
- Median cubital vein. The basilic and cephalic veins are joined at the inductive attribute of the elbow by the median cubital vein, often chosen as the site for blood removal for the purpose of blood testing.
- Subclavian vein. The subclavian vein receives venous blood from the arm through the axillary vein and from the peel and muscles of the head through the external jugular vein.
- Vertebral vein. The vertebral vein drains the posterior role of the head.
- Internal jugular vein. The internal jugular vein drains the dural sinuses of the encephalon.
- Brachiocephalic veins. The right and left brachiocephalic veins are large veins that receive venous drainage from the subclavian, vertebral, and internal jugular veins on their respective sides.
- Azygos vein. The azygos vein is a single vein that drains the thorax and enters the superior vena cava but before it joins the heart.
Veins Draining into the Junior Vena Cava
The inferior vena cava, which is much longer than the superior vena cava, returns claret to the heart from all body regions below the diaphragm.
- Tibial veins. The anterior and posterior tibial veins and the fibular vein drain the leg; the posterior tibial veins becomes the popliteal vein at the knee joint and then the femoral vein in the thigh; the femoral vein becomes the external iliac vein as it enters the pelvis.
- Great saphenous veins. The dandy saphenous veins are the longest veins in the body; they brainstorm at the dorsal venous arch in the human foot and travel up the medial aspect of the leg to empty into the femoral vein in the thigh.
- Mutual iliac vein. Each common iliac vein is formed by the union of the external iliac vein and the internal iliac vein which drains the pelvis.
- Gonadal vein. The right gonadal vein drains the right ovary in females and the correct testicles in males; the left gonadal veins empties into the left renal veins superiorly.
- Renal veins. The right and left renal veins bleed the kidneys.
- Hepatic portal vein. The hepatic portal vein is a unmarried vein that drains the digestive tract organs and carries this claret through the liver before it enters the systemic circulation.
- Hepatic veins. The hepatic veins bleed the liver.
Physiology of the Heart
As the heart beats or contracts, the blood makes continuous circular trips- into and out of the heart, through the rest of the body, and then dorsum to the middle- only to be sent out again.
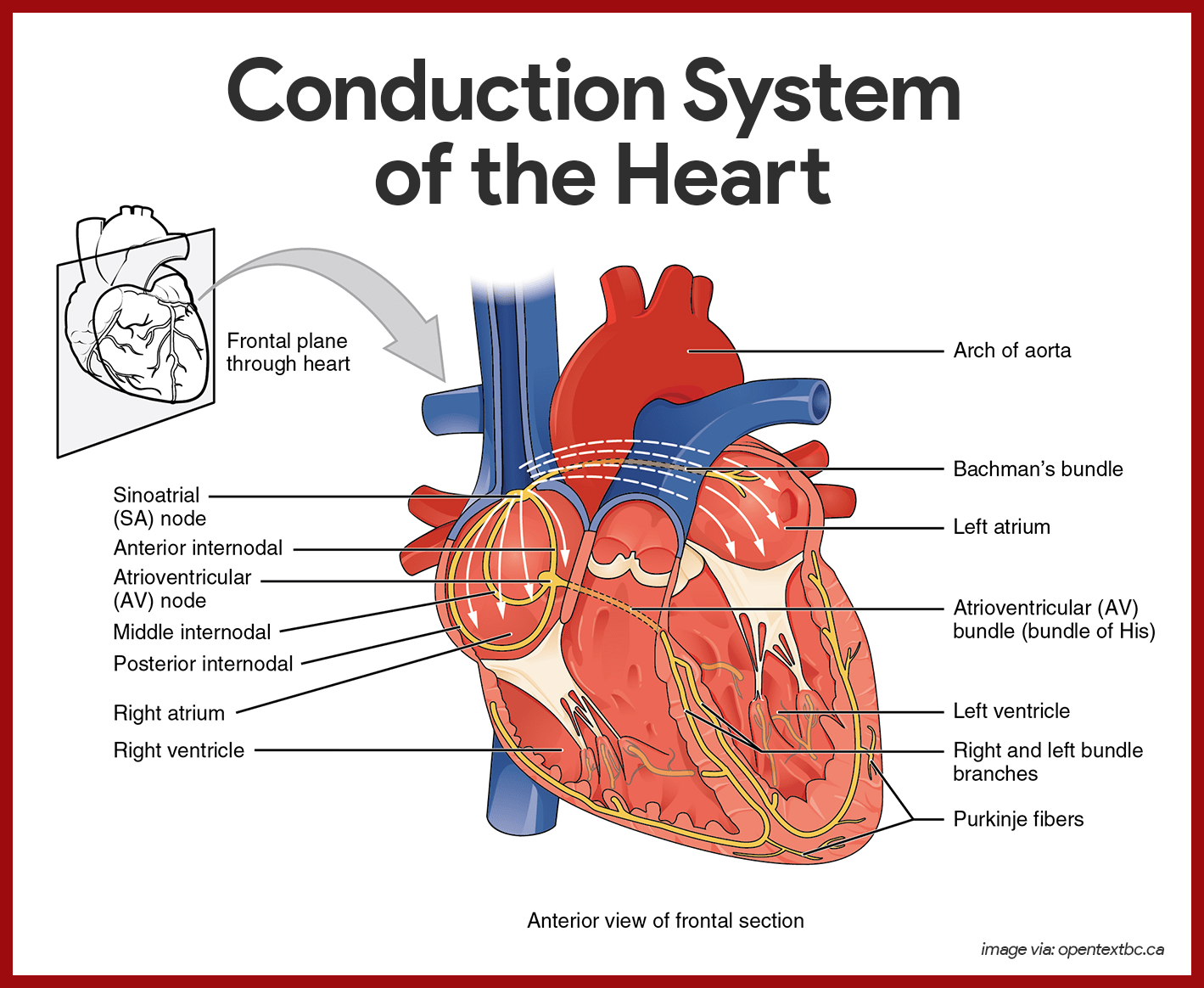
Intrinsic Conduction System of the Middle
The spontaneous contractions of the cardiac muscle cells occurs in a regular and continuous way, giving rhythm to the heart.
- Cardiac musculus cells. Cardiac muscle cells can and practise contract spontaneously and independently, even if all nervous connections are severed.
- Rhythms. Although cardiac muscles tin beat independently, the muscle cells in the different areas of the middle take different rhythms.
- Intrinsic conduction system. The intrinsic conduction system, or the nodal organisation, that is built into the heart tissue sets the basic rhythm.
- Limerick. The intrinsic conduction system is composed of a special tissue found nowhere else in the trunk; information technology is much like a cross betwixt a musculus and nervous tissue.
- Part. This system causes heart muscle depolarization in only one management- from the atria to the ventricles; it enforces a contraction rate of approximately 75 beats per minute on the heart, thus the heart beats equally a coordinated unit.
- Sinoatrial (SA) node. The SA node has the highest rate of depolarization in the whole system, and so it tin can start the beat and set the pace for the whole heart; thus the term "pacemaker".
- Atrial contraction. From the SA node, the impulse spread through the atria to the AV node, and so the atria contract.
- Ventricular contraction. It then passes through the AV bundle, the bundle branches, and the Purkinje fibers, resulting in a "wringing" contraction of the ventricles that begins at the heart apex and moves toward the atria.
- Ejection. This contraction effectively ejects claret superiorly into the large arteries leaving the middle.
The Pathway of the Conduction System
The conduction system occurs systematically through:
- SA node. The depolarization moving ridge is initiated past the sinoatrial node.
- Atrial myocardium. The wave then successively passes through the atrial myocardium.
- Atrioventricular node. The depolarization wave so spreads to the AV node, and then the atria contract.
- AV package. It and so passes rapidly through the AV bundle.
- Bundle branches and Purkinje fibers. The wave then continues on through the right and left bundle branches, and and so to the Purkinje fibers in the ventricular walls, resulting in a contraction that ejects claret, leaving the eye.
Cardiac Bike and Heart Sounds
In a good for you heart, the atria contract simultaneously, then, as they start to relax, wrinkle of the ventricles begin.
- Systole. Systole means heart wrinkle.
- Diastole. Diastole means heart relaxation.
- Cardiac cycle. The term cardiac cycle refers to the events of one consummate heart crush, during which both atria and ventricles contract and then relax.
- Length. The average eye beats approximately 75 times per minute, so the length of the cardiac bike is normally about 0.8 second.
- Mid-to-belatedly diastole. The cycle starts with the centre in complete relaxation; the force per unit area in the heart is low, and blood is flowing passively into and through the atria into the ventricles from the pulmonary and systemic circulations; the semilunar valves are closed, and the AV valves are open; then the atria contract and force the blood remaining in their chambers into the ventricles.
- Ventricular systole. Shortly after, the ventricular contraction begins, and the pressure level within the ventricles increases apace, closing the AV valves; when the intraventricular pressure level is higher than the pressure in the large arteries leaving the centre, the semilunar valves are forced open, and blood rushes through them out of the ventricles; the atria are relaxed, and their chambers are again filling with claret.
- Early diastole. At the end of systole, the ventricles relax, the semilunar valves snap shut, and for a moment the ventricles are completely closed chambers; the intraventricular pressure level drops and the AV valves are forced open; the ventricles over again brainstorm refilling rapidly with blood, completing the cycle.
- Kickoff heart audio. The commencement centre sound, "lub", is acquired past the closing of the AV valves.
- Second heart audio. The second heart sound, "dub", occurs when the semilunar valves shut at the end of systole.
Cardiac Output
Cardiac output is the amount of blood pumped out by each side of the heart in 1 minute. It is the production of the heart charge per unit and the stroke volume.
- Stroke volume. Stroke volume is the volume of claret pumped out by a ventricle with each heartbeat.
- Regulation of stroke volume. According to Starling's police force of the eye, the disquisitional gene controlling stroke book is how much the cardiac muscle cells are stretched just before they contract; the more they are stretched, the stronger the wrinkle volition be; and anything that increases the volume or speed of venous return as well increases stroke volume and strength of wrinkle.
- Factors modifying bones heart charge per unit.The most of import external influence on center rate is the activity of the autonomic nervous organization, as well as concrete factors (historic period, gender, exercise, and body temperature).
Physiology of Apportionment
A fairly good indication of the efficiency of a person's circulatory system can be obtained past taking arterial blood and blood pressure measurements.
Cardiovascular Vital Signs
Arterial pulse pressure and blood pressure level measurements, along with those of respiratory rate and torso temperature, are referred to collectively every bit vital signs in clinical settings.
- Arterial pulse. The alternate expansion and recoil of an artery that occurs with each shell of the left ventricle creates a pressure moving ridge-a pulse- that travels through the unabridged arterial system.
- Normal pulse rate. Normally, the pulse charge per unit (force per unit area surges per minute) equals the heart charge per unit, and then the pulse averages 70 to 76 beats per minute in a normal resting person.
- Pressure points. There are several clinically important arterial pulse points, and these are the same points that are compressed to stop blood menstruum into distal tissues during hemorrhage, referred to as pressure points.
- Blood pressure. Claret pressure is the force per unit area the claret exerts confronting the inner walls of the blood vessels, and it is the force that keeps claret circulating continuously fifty-fifty between heartbeats.
- Claret pressure gradient. The pressure is highest in the large arteries and continues to drop throughout the systemic and pulmonary pathways, reaching either nil or negative pressure level at the venae cavae.
- Measuring claret force per unit area. Because the heart alternately contracts and relaxes, the off-and-on flow of the claret into the arteries causes the blood pressure level to rise and autumn during each beat, thus, ii arterial blood pressure measurements are usually made: systolic pressure (the pressure level in the arteries at the superlative of ventricular contraction) and diastolic pressure (the pressure when the ventricles are relaxing).
- Peripheral resistance. Peripheral resistance is the amount of friction the blood encounters equally it flows through the claret vessels.
- Neural factors. The parasympathetic division of the autonomic nervous arrangement has picayune or no effect on blood force per unit area, but the sympathetic division has the major activity of causing vasoconstriction or narrowing of the claret vessels, which increases claret pressure.
- Renal factors. The kidneys play a major function in regulating arterial claret pressure by altering blood volume, and then when blood pressure increases beyond normal, the kidneys permit more than water to leave the body in the urine, and then blood book decreases which in turn decreases blood pressure.
- Temperature. In general, cold has a vasoconstricting effect, while heat has a vasodilating issue.
- Chemicals. Epinephrine increases both heart charge per unit and claret pressure; nicotine increases blood force per unit area past causing vasoconstriction; booze and histamine cause vasodilation and decreased claret pressure.
- Diet. Although medical opinions tend to change and are at odds from fourth dimension to fourth dimension, it is generally believed that a diet low in salt, saturated fats, and cholesterol help to forbid hypertension, or high claret pressure.
Blood Apportionment Through the Heart
The correct and left sides of the center work together in achieving a shine flowing claret circulation.
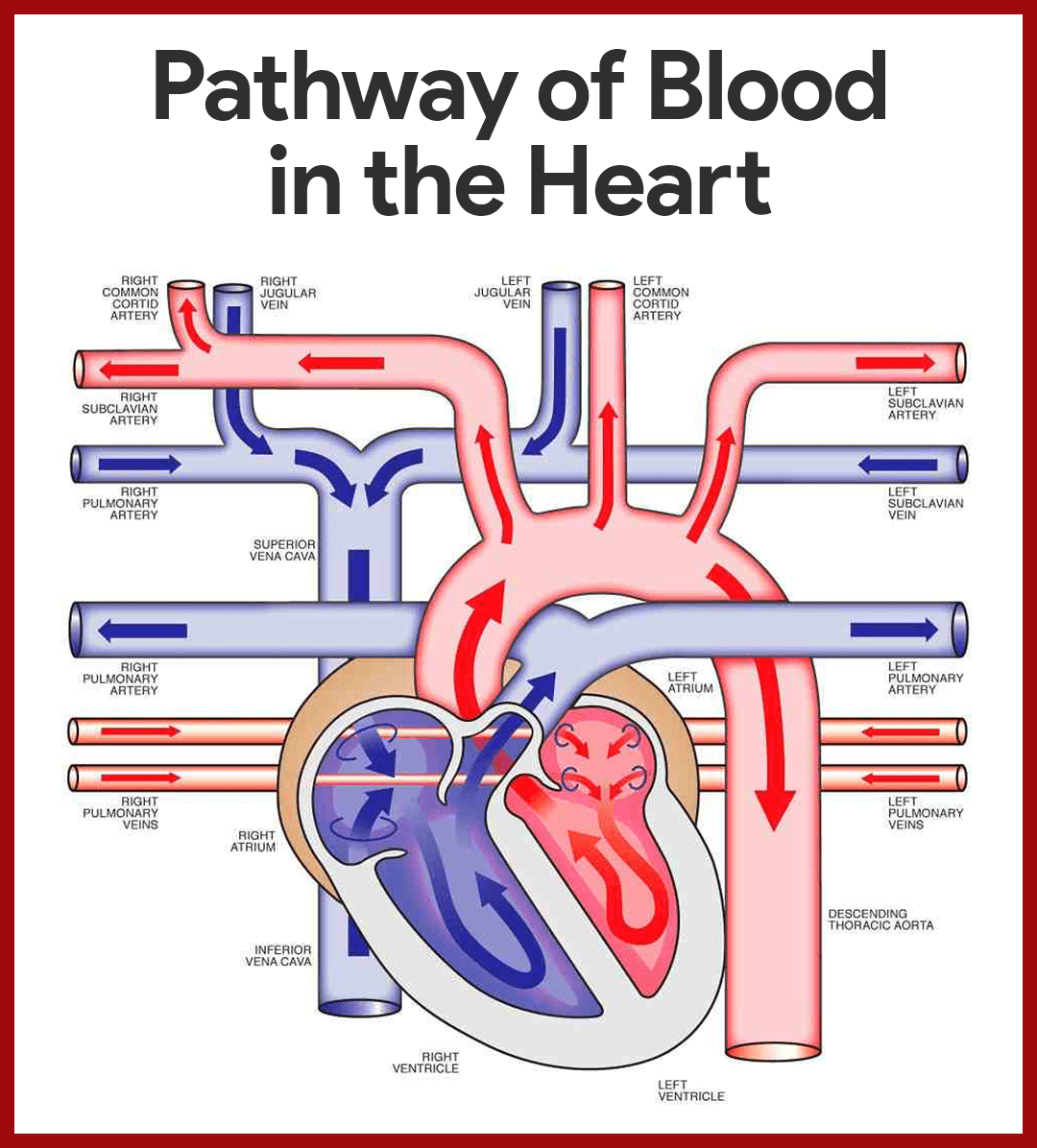
- Archway to the heart. Claret enters the heart through two large veins, the inferior and superior vena cava, emptying oxygen-poor blood from the trunk into the correct atrium of the heart.
- Atrial contraction. As the atrium contracts, blood flows from the correct atrium to the right ventricle through the open up tricuspid valve.
- Closure of the tricuspid valve. When the ventricle is full, the tricuspid valve shuts to prevent claret from flowing astern into the atria while the ventricle contracts.
- Ventricle contraction. Every bit the ventricle contracts, blood leaves the heart through the pulmonic valve, into the pulmonary artery and to the lungs where it is oxygenated.
- Oxygen-rich blood circulates. The pulmonary vein empties oxygen-rich blood from the lungs into the left atrium of the centre.
- Opening of the mitral valve. As the atrium contracts, blood flows from your left atrium into your left ventricle through the open mitral valve.
- Prevention of backflow. When the ventricle is full, the mitral valve shuts. This prevents blood from flowing astern into the atrium while the ventricle contracts.
- Blood flow to systemic circulation. Every bit the ventricle contracts, blood leaves the heart through the aortic valve, into the aorta and to the torso.
Capillary Commutation of Gases and Nutrients
Substances tend to move to and from the trunk cells according to their concentration gradients.
- Capillary network. Capillaries form an intricate network amongst the body's cells such that no substance has to diffuse very far to enter or get out a prison cell.
- Routes. Basically, substances leaving or entering the blood may have one of iv routes across the plasma membranes of the unmarried layer of endothelial cells forming the capillary wall.
- Lipid-soluble substances. As with all cells, substances tin can lengthened directly through their plasma membranes if the substances are lipid-soluble.
- Lipid-insoluble substances. Certain lipid-insoluble substances may enter or go out the blood and/or pass through the plasma membranes within vesicles, that is, past endocytosis or exocytosis.
- Intercellular clefts. Limited passage of fluid and small solutes is allowed by intercellular clefts (gaps or areas of plasma membrane not joined by tight junctions), and so near of our capillaries have intercellular clefts.
- Fenestrated capillaries. Very costless passage of small solutes and fluid is allowed past fenestrated capillaries, and these unique capillaries are found where absorption is a priority or where filtration occurs.
Practice Quiz: Cardiovascular Organization
Here's a ten-item quiz about the written report guide. Please visit our nursing test banking concern page for more NCLEX practice questions.
ane. Specialized jail cell membrane structures that decrease electrical resistance between the cells allowing activeness potentials to pass efficiently from ane prison cell to adjacent cells are the:
A. Extensive capillary network
B. Intercalated disks
C. Mitochondria
D. Gap junctions
ane. Answer: D. Gap junctions
D:Gap junctions are a specialized intercellular connexion between a multitude of animal cell-types. They directly connect the cytoplasm of two cells, which allows diverse molecules, ions and electric impulses to directly pass through a regulated gate between cells.
A: All-encompassing capillary networks allows abundant supply of oxygen and nutrients on tissues such as skeletal muscle, liver, and kidney.
B: Intercalated disks support synchronized contraction of cardiac tissue. They occur at the Z-line of the sarcomere and tin be visualized easily when observing a longitudinal section of the tissue.
C: Mitochondrion is an organelle found in large numbers in most cells, in which the biochemical processes of respiration and energy production occur.
2. Consummate the diagram so that information technology will show the correct route of claret in the heart.

A. (ane) Tricuspid Valve, (ii) Aortic Valve, (3) Pulmonary Circulation, (4) Mitral Valve, (5) Pulmonic Valve
B. (1) Mitral Valve, (2) Pulmonic Valve, (three) Pulmonary Circulation, (4) Tricuspid Valve, (5) Aortic Valve
C. (1) Mitral Valve, (2) Aortic Valve, (3) Pulmonary Circulation, (iv) Tricuspid Valve, (5) Pulmonic Valve
D. (1) Tricuspid Valve, (2) Pulmonic Valve, (iii) Pulmonary Circulation, (4) Mitral Valve, (5) Aortic Valve
2. Reply: D. (1) Tricuspid Valve, (2) Pulmonic Valve, (three) Pulmonary Circulation, (four) Mitral Valve, (5) Aortic Valve
Blood enters the eye through two large veins, the inferior and superior vena cava, emptying oxygen-poor blood from the trunk into the right atrium. As the atrium contracts, blood flows from your right atrium into your right ventricle through the open tricuspid valve. When the ventricle is full, the tricuspid valve shuts. This prevents blood from flowing backward into the right atrium while the ventricle contracts. Every bit the ventricle contracts, blood leaves the eye through the pulmonic valve, into the pulmonary avenue and to the lungs, where it is oxygenated. The oxygenated blood and then returns to the centre through the pulmonary veins. The pulmonary veins empty oxygen-rich blood from the lungs into the left atrium. Equally the atrium contracts, blood flows from your left atrium into your left ventricle through the open mitral valve. When the ventricle is full, the mitral valve shuts. This prevents blood from flowing astern into the atrium while the ventricle contracts. Equally the ventricle contracts, blood leaves the heart through the aortic valve, into the aorta, and to the body.
3. Information technology is considered as the bluntly rounded portion of the heart
A. Aorta
B. Apex
C. Base
D. Pericardium
3. Answer: B. Apex
B: The blunt, rounded point of the heart is the noon.
A: The aorta is the largest avenue that carries blood from the left ventricle to the body.
C: The larger, flat portion at the opposite is the base.
D. The pericardium is besides chosen the pericardial sac.It has a fibrous outer layer and a sparse inner layer that surrounds the heart.
4. Which upshot will NOT occur during depolarization stage?
A. Na+ channels open
B. Ca+ channels open up
C. K+ channels open up
D. None of the above
iv. Respond: C. Chiliad+ channels open
Na+ channels open, increasing the permeability of the jail cell membrane to Na+. Sodium ions so diffuse into the cell, causing depolarization. This causes K+ channels to close chop-chop, decreasing the permeability of the prison cell membrane to 1000+. The decreased diffusion of K+ out of the prison cell also causes depolarization. Ca2+ channels slowly open, increasing the permeability of jail cell membrane to Ca2+. Calcium ions and then diffuse into the cell and cause depolarization.
five. Which of these statements regarding the conduction system of the heart is Truthful?
A. The sinoatrial (SA) node of the eye acts as the pacemaker.
B. The SA node is located on the upper wall of the left atrium.
C. The AV node conducts action potentials rapidly through it.
D. Action potentials are carried slowly through the atrioventricular bundle.
5. Respond: A. The sinoatrial (SA) node of the eye acts as the pacemaker.
A: The SA node is the heart's natural pacemaker.
B: The SA node consists of a cluster of cells that are situated in the upper part of the wall of the right atrium (the right upper chamber of the middle).
C: When action potentials attain the AV node, they spread slowly through it.
D: Action potentials pass slowly through the atrioventricular node.
6. In a normal electrocardiogram (ECG or EKG),
A. The P wave results from repolarization of the atria.
B. The QRS complex results from depolarization of the ventricles.
C. The T wave represents repolarization of the auricles.
D. During the P-R interval, the ventricle contract.
six. Answer: B. The QRS complex results from depolarization of the ventricles.
B: The QRS complex consists of three individual waves: the Q, R, and S waves. The QRS complex results from depolarization of the ventricles, and the beginning of the QRS complex precedes ventricular contraction.
A: The P wave results from depolarization of the atrial myocardium, and the get-go of the P wave precedes the onset of atrial contraction.
C: The T wave represents the repolarization of the ventricles, and the beginning of the T wave precedes ventricular relaxation.
D: During the P-R interval, the atria contract and begin to relax.
7. During the Ventricular Systole, atrioventricular valves open up, semilunar valves close. The statement is:
A. True
B. Fake
C. Partially true
D. Partially fake
7. Answer: B. Faux
During ventricular systole, wrinkle of the ventricles causes pressure level in the ventricle to increase. Almost immediately the AV valves close (the first heart audio). The pressure in the ventricle continues to increment. Connected ventricular wrinkle causes the pressure in the ventricle to exceed in the pulmonary trunk and aorta. As a issue, the semilunar are forced open and blood is ejected into the pulmonary trunk and aorta.
8. This sound is produced during the closure of the semilunar valves.
A. lubb
B. dupp
C. lubb dupp
D. lubb duppshhh
eight. Answer: B. dupp
B: The 2d heart sound can be represented past dupp. It occurs at the beginning of ventricular diastole and results from closure of the semilunar valves.
A: The commencement heart audio can be represented by the syllable lubb. Information technology occurs at the beginning of ventricular systole and results from closure of the AV valves.
9. Which of these statements correctly applies to intrinsic regulation of the middle?
A. Starling's law of the heart has a major influence on cardiac output.
B. As venous render increases, cardiac output decreases.
C. In response to stretch, cardiac muscle fibers contract with less force.
D. In response to stretch, there is a slight decrease in heart rate.
ix. Answer: A. Starling'south law of the heart has a major influence on cardiac output.
A: The relationship between preload and stroke volume is chosen Starling's law of the heart.
B: As venous return increased, resulting in an increased preload, cardiac output increases.
C: In response to increased preload, cardiac muscle fibers contract with greater force.
D: In response to stretch, there is a slight increment in heart rate.
10. Repolarization of the ventricles is shown as the __________ on an ECG or EKG.
A. P wave
B. P-Q or P-R interval
C. QRS complex
D. Q-T interval
Eastward. T wave
x. Respond: East. T wave
E: The T wave represents the repolarization of the ventricles, and the beginning of the T wave precedes ventricular relaxation.
A: The P moving ridge results from depolarization of the atrial myocardium, and the beginning of the P wave precedes the onset of atrial contraction.
B: The time between the beginning of the P wave and the offset of the QRS complex is the PQ interval, commonly chosen the PR interval because the Q wave is very small. During the PR interval, the atria contract and begin to relax.
C: The QRS complex consists of iii individual waves: the Q, R, and Southward waves. The QRS circuitous results from depolarization of the ventricles, and the beginning of the QRS circuitous precedes ventricular wrinkle.
D: The QT interval extends from the beginning of the QRS complex to the end of the T wave and represents the length of time required for ventricular depolarization and repolarization.
Source: https://nurseslabs.com/cardiovascular-system-anatomy-physiology/
0 Response to "Review Sheet 31 Conduction System of the Heart"
Post a Comment